Fracture Surgery In Noida - Types Of Fractures, Surgical Treatment, And Recovery
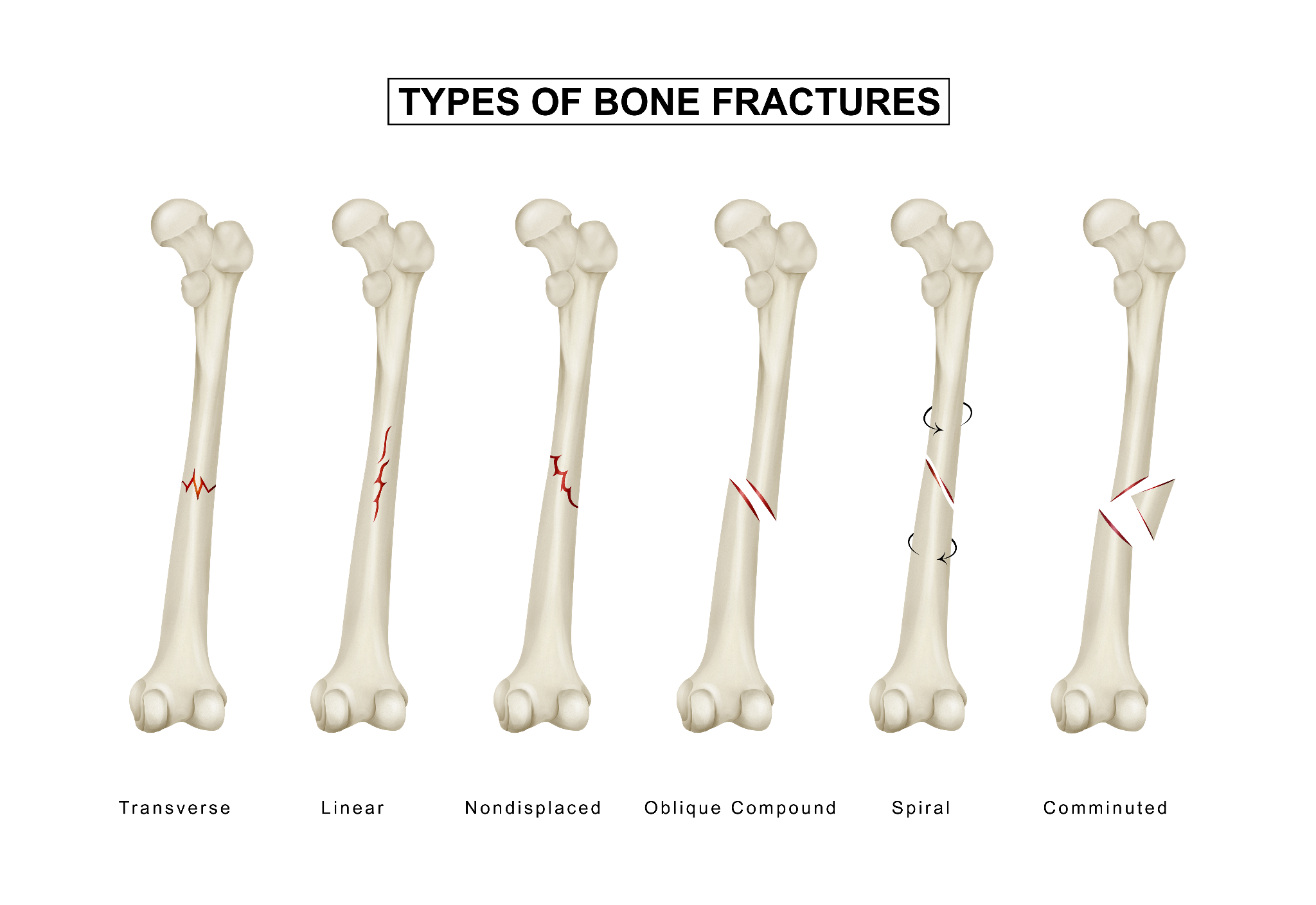
An infographic illustrating different types of bone fractures, including simple, compound, greenstick, and comminuted fractures for easy understanding.
A fracture, a broken bone, is one of the most common reasons people visit an orthopedic surgeon in Noida and Greater Noida. Road traffic accidents, sports injuries, falls in the elderly, and workplace injuries all produce fractures at a significant rate in a city and region as populous as Delhi NCR.
But "fracture" covers an enormous range of presentations from a hairline crack in a metatarsal that heals with rest and supportive footwear, to a comminuted (shattered) femur shaft that requires complex surgical fixation and months of recovery. The treatment approach is not the same across the spectrum.
This guide explains when fractures need surgery, what surgical fracture treatment actually involves, and what recovery looks like for patients in Noida and their families who are trying to understand what they're dealing with.
Not All Fractures Need Surgery
The first point worth establishing clearly: the majority of fractures in clinical practice are managed without surgery. Conservative (non-surgical) management, casting, splinting, bracing, or simple immobilisation, is appropriate for:
- Undisplaced Fractures (the broken ends are still in good alignment)
- Stable fractures that won't shift with normal healing
- Fractures where the risks of surgery outweigh the benefits (such as certain fractures in very elderly patients with multiple comorbidities)
- Stress fractures (hairline fractures from repetitive loading) in most locations
- Most clavicle (collarbone) fractures
- Most rib fractures
- Most toe fractures
The surgical decision is made when conservative management would leave the bone in unacceptable alignment, or when surgical fixation would produce significantly better functional outcomes than conservative treatment.
Types Of Fractures - Understanding The Terminology
Before discussing treatment, understanding how fractures are classified helps in understanding why different injuries are managed differently. By displacement:
- Undisplaced: The bone is broken, but the fragments have not shifted position. Conservative management is usually possible.
- Displaced: The fragments have moved out of alignment. Surgical correction is usually needed.
By pattern:
- Transverse: A clean horizontal break across the bone, typically from a direct blow.
- Oblique: An angled fracture, common with twisting forces.
- Spiral: A helical fracture pattern, classic for rotational injuries (a twisting fall).
- Comminuted: The bone has shattered into multiple fragments, typically from high-energy injuries (road accidents, falls from height).
- Segmental: Two fracture lines creating an isolated segment of bone.
- Avulsion: A fragment of bone pulled off by a ligament or tendon attachment.
By skin status:
- Closed fracture: The skin over the fracture is intact. Most fractures.
- Open (compound) fracture: The bone has pierced through the skin, or there is a wound communicating with the fracture. This is a surgical emergency; the risk of bone infection (osteomyelitis) is high, and the wound must be surgically cleaned and the fracture stabilised within hours.
By involvement of the joint:
- Intra-articular fracture: The fracture line enters a joint surface. These are particularly important to address if the joint surface heals in poor alignment, as the result is early post-traumatic arthritis. Surgical precision in restoring joint congruity is critical.
When Is Fracture Surgery Needed?
The general criteria for surgical fixation of a fracture:
- Displaced fractures that cannot be adequately reduced (put back into alignment) and held in position with a cast
- Intra-articular fractures to restore the joint surface precisely.
- Open fractures - Urgent surgery for wound cleaning (debridement) and fracture stabilisation.
- Fractures with neurovascular injury - Emergency exploration and stabilisation
- Pathological fractures - Fractures through abnormal bone (tumour, severe osteoporosis) that require stabilisation.
- Hip fractures in elderly patients - Where surgical fixation allows early walking, reducing the catastrophic complications of prolonged bed rest.
- Fractures that fail to unite with conservative treatment (non-union).
- Multiple fractures - Polytrauma patients where early fracture stabilisation reduces overall complications.
- Fractures in certain anatomical locations where conservative management reliably produces poor outcomes.
Surgical Methods For Fracture Fixation
1. Open Reduction And Internal Fixation (ORIF)
The most commonly performed fracture surgery. The operation has two components:
- Open reduction: The fracture is exposed through a surgical incision, and the bone fragments are manually repositioned into correct anatomical alignment.
- Internal fixation: Metal implant plates, screws, rods, or combinations are used to hold the bone in position while it heals.
Plates and screws: Metal plates contoured to the bone shape are applied and secured with screws. Excellent for many periarticular fractures (around joints) and shaft fractures where a plate provides stable fixation. Modern locking plates lock the screws into the plate, providing greater stability, particularly important in osteoporotic bone.
Intramedullary nailing (IM Nail): A metal rod is inserted into the hollow canal of a long bone (femur, tibia, humerus) and locked with cross-screws above and below the fracture. This is the preferred method for shaft fractures of the femur and tibia. It allows immediate weight-bearing in many cases and has very high success rates.
Cannulated screws: Hollow screws used for specific fracture types, particularly femoral neck fractures in younger patients and certain other periarticular fractures.
K-wires (Kirschner wires): Thin metal wires used for temporary fixation or for certain smaller bone fractures (fingers, distal radius in children).
2. Closed Reduction And Internal Fixation (CRIF)
The fracture is reduced (realigned) without directly opening the fracture site using image intensification (X-ray guidance in the OT), and then fixed with nails or screws placed through small incisions. Less tissue disruption than open surgery. Used for specific fracture types amenable to this approach.
3. External Fixation
A frame of metal pins is inserted into the bone above and below the fracture, connected externally by bars. The bone is held in alignment by the external frame rather than by implants inside the body.
When external fixation is used:
- Open fractures as temporary stabilisation before definitive surgery, particularly when the wound is contaminated.
- Highly comminuted fractures where internal fixation is not yet feasible.
- Fractures with severe soft tissue damage.
- Fractures in patients who are not yet medically stable for prolonged internal fixation surgery (damage control orthopaedics).
4. Intramedullary Nailing (Long Bone Shaft Fractures)

A patient using crutches and a knee brace while walking under medical supervision in a rehabilitation setting.
The most important technique for fractures of the femur shaft (thigh bone), tibial shaft (shin bone), and humeral shaft (upper arm). A metal rod is introduced into the medullary canal of the bone, typically from one end (the knee end for femoral nails; the knee end or ankle end for tibial nails). Cross-locking screws at each end of the nail prevent rotation and shortening.
Advantages of IM nailing:
- Minimal soft tissue disruption at the fracture site (the nail is introduced from a distant entry point, not from the fracture itself)
- Strong, flexible fixation that shares load with the healing bone
- Allows early weight-bearing in many cases
- Very high union rates
Common Fractures In Noida - What Treatment Looks Like
1. Hip Fractures (Neck Of Femur And Intertrochanteric)
One of the most common and most serious fractures seen in Noida's elderly population. Hip fractures typically occur after a fall, sometimes even a relatively minor one, in osteoporotic patients. Why hip fractures are a medical emergency:
The 1-year mortality rate after hip fracture is approximately 20–30% in elderly patients without timely surgical treatment. Prolonged bed rest waiting for surgery leads to pulmonary embolism, pneumonia, pressure sores, urinary infections, and progressive deconditioning, all of which increase mortality.
International guidelines recommend hip fracture surgery within 24-48 hours of hospital admission. Delaying surgery beyond 48 hours is associated with significantly higher complication and mortality rates.
Surgical options:
- Dynamic Hip Screw (DHS) / Cannulated screws: For undisplaced and some displaced femoral neck fractures in younger patients — preserves the patient's own femoral head.
- Hemiarthroplasty (partial hip replacement): For displaced femoral neck fractures in elderly patients over 70, the damaged femoral head is replaced with a metal prosthesis. Allows immediate full weight-bearing. Recovery is faster than internal fixation in elderly patients.
- Intramedullary nail (PFNA, Gamma nail): For intertrochanteric fractures (breaks at the junction of the neck and shaft), these heal well with IM nailing in most cases.
2. Wrist Fractures (Distal Radius Fracture / Colles Fracture)
The most common fracture in adults overall, particularly in women with osteoporosis and in young people after falls. A fall on an outstretched hand fractures the radius just above the wrist.
Management:
- Undisplaced and minimally displaced fractures: Cast immobilisation for 4-6 weeks.
- Displaced fractures that cannot be held in a cast: Surgical fixation is most commonly a volar locking plate (ORIF through a palm-side incision) that provides excellent stability and allows early hand movement.
- Very comminuted fractures: External fixation.
3. Ankle Fractures
Ankle fractures typically involve the medial malleolus (inner ankle), lateral malleolus (outer ankle, the fibula), or both (bimalleolar fracture) from rolling or twisting injuries. Severe injuries can involve the posterior malleolus as well (trimalleolar fractures).
Management:
- Isolated undisplaced lateral malleolus fractures with a stable ankle joint: Conservative in a boot/cast.
- Displaced bimalleolar and trimalleolar fractures: ORIF with plates and screws. Restoring the ankle joint congruity is essential; even a small displacement leads to early ankle arthritis.
4. Tibial Shaft Fractures
High-energy fractures are typically caused by road accidents in Noida, where two-wheeler accidents are common. The tibia has poor soft tissue coverage, making soft tissue management a significant component of treatment.
Management: Intramedullary nailing is the standard treatment, which allows early weight-bearing and has excellent union rates. Open tibial fractures require urgent wound management alongside stabilisation.
5. Femoral Shaft Fractures
A major long bone fracture typically from high-energy trauma. Significant blood loss can occur from bleeding into the thigh.
Management: Antegrade intramedullary femoral nailing, inserting the nail from the proximal femur, in the operating room under X-ray guidance. Modern long femoral nails produce excellent outcomes with early mobilisation.
6. Clavicle (Collarbone) Fractures
Extremely common from falls, sports contact, and road accidents. Historically managed conservatively (sling for 4–6 weeks), but surgical fixation with a plate is now preferred for significantly displaced midshaft fractures in active adults, as it reduces malunion rates and produces faster recovery.
7. Finger And Hand Fractures
Very common in sports and workplace injuries. Management ranges from buddy-taping (for stable phalangeal fractures) to surgical fixation with K-wires, screws, or plates for unstable or intra-articular fractures. Accurate treatment is important, as malunion of finger fractures causes significant functional impairment.
Recovery After Fracture Surgery
Recovery depends enormously on which bone was fractured, the type of fixation, the patient's age and health, and the quality of rehabilitation. General principles:
- Most operatively fixed fractures allow earlier mobilisation than conservatively managed ones. This is one of the key advantages of surgical fixation.
- Physiotherapy begins as soon as the patient's condition allows. For hip fracture surgery, this means walking the next day.
- Weight-bearing guidance is specific to the fracture type and fixation. Your surgeon will specify when you can bear weight and how much.
- Bone healing takes 6-12 weeks for most fractures, longer for large bone fractures (femur: 12–16 weeks) and for patients with osteoporosis.
- Full functional recovery of muscle strength, range of motion, and confidence takes longer than bone union, often 3–6 months.
Fracture Surgery In Noida - Dr. Mayank Chauhan At Prakash Hospital
Dr. Mayank Chauhan, Senior Orthopedic Surgeon at Prakash Hospital, Sector 33, Noida, manages the full spectrum of fracture care from acute trauma surgery to delayed presentations and fractures requiring revision.
Prakash Hospital provides:
- 24-hour emergency fracture management capability.
- Modern OT infrastructure with image intensification (C-arm fluoroscopy).
- A full range of fracture fixation implants, plates, nails, screws, and external fixators.
- Post-operative physiotherapy and rehabilitation support.
- Close follow-up with serial X-rays to confirm healing.
For families in Noida and Greater Noida dealing with an acute fracture, particularly hip fractures in elderly relatives, early contact with Dr. Chauhan's team allows prompt surgical planning. To book a consultation or for urgent fracture evaluation, call the number listed on the website.
The Bottom Line

A fractured leg
Fracture surgery is not "one size fits all." The right operation for a displaced intra-articular ankle fracture is different from the right operation for a femoral shaft fracture, which is different again from the management of a hip fracture in an 80-year-old. The surgeon's experience with specific fracture types, access to the right implants, and quality of post-operative rehabilitation all affect outcome.
For fractures in Noida and Greater Noida, whether from road accidents, sports injuries, or falls, prompt evaluation and appropriate management (surgical or conservative) is essential to maximise functional recovery. To consult Dr. Mayank Chauhan, Senior Orthopedic Surgeon in Noida, call the number listed on the website.

















